You would highly regard our five-star Central Coast Home Health RNs. Such caring, confident, calm, and competent professionals who put the needs of the patient first. Yesterday our nurse provided superior, easy-to-follow, hands-on instruction in the use and maintenance of my new high-tech MIC-KEY. Using a 60 ml syringe, the nurse handled the 60 ml pre-flush of water into my port and encouraged Jon to take over, administering 5.5 ounces of formula followed by a post-flush of 90 ml water. Note: We use reverse osmosis (RO) water—the same water we drink, cook with, give our dogs and hens. The plan is to slowly introduce the prescribed Kate Farms formula to allow my digestive system time to become acquainted with it—hopefully preventing digestive disturbance. We’re aiming for absolute success!
So thankful Jon is able and willing to assist. Also grateful the process doesn’t involve needles—Jon is squeamish when it comes to needles. However, he is comfortable attaching the extensions and tubes to the MIC-KEY which is comparable to some challenging and intricate plumbing projects he’s tackled for us.
At this point in time, the MIC-KEY is not my only way to receive nutrition. The purpose of having the feeding tube surgically inserted now is this: While I can still eat via mouth, it allows me time to adjust and become accustomed to using the MIC-KEY for caloric intake as well as staying sufficiently hydrated. My water consumption isn’t what it should be because swallowing thin liquids isn’t easy. Even though I’m still able to eat, it is an arduous endeavor. It takes far longer to chew my food than pre-ALS. I can’t handle soup with mixed textures, mac and cheese, pasta salad, or an In-N-Out burger. Too bad for me but more for you! Well, not all of you. I realize the vegetarians among us won’t be looking for an In-N-Out burger; although, I do know vegetarians who order ‘the works’ minus the beef, and love it! And my vegan friends won’t miss mac and cheese. My soup must be puréed to one smooth consistency. Same applies to mac and cheese. Haven’t tried that with an In-N-Out burger nor do I plan to.
A Nostalgic Trip Down Memory Lane My dad would be happy to hear this. Loading us in his trusty Volkswagen bus, he loved taking us to one of the original In-N-Out drive-throughs in Pasadena on East Foothill Boulevard. That was way before In-N-Out started adding dining rooms. All the original In-N-Outs were strictly drive-throughs. To this day, their location on East Foothill Boulevard still is drive-through only! My dad would be aghast if he saw his daughter put one of those tasty burgers in her blender and . . . you would probably look the other way, too!
When solids (e.g., carrots, celery, potatoes, zucchini, olives, etc.) separate from liquids in my mouth and head for the back of my throat prematurely, that poses a serious choking hazard. It takes a lot of concentration and focus just to eat. No distractions! Evenings are the most difficult because I’m already tired from the day—resulting in even greater fatigue from chewing and swallowing. What used to take me 10 minutes to consume easily turns into 45 minutes. By the time I finish . . . if I finish . . . I’m completely worn out and may not have consumed enough calories.
So far, I haven’t used my MIC-KEY. Here’s why: At UCSF, the procedure for surgically inserting a feeding tube mandates a standard overnight stay in the hospital. That hospital sends patients home with a “starter kit” including hoses, syringes, connecter extenders, liquid food, etc. UCSF assumed this to be the protocol followed by French Hospital. Nope. French utilizes outpatient day surgery for feeding tube placements. I was discharged Thursday afternoon with zero supplies. The UCSF registered dietician and my amazing home health RNs have scrambled unbelievably to get me what I need; but due to proliferation of the not-so-helpful-nor-exciting game of phone tag, there have been numerous snags delaying deliveries. Add the Thanksgiving extended weekend . . . Good thing I’m still able to get nutrition via my mouth! Today we received a couple of supply deliveries with more en route. We anticipate beginning tube feeding instructional training tomorrow (Wednesday, November 27).
Sailed through the placement of a G-feeding tube. Based on first-hand participation, Thursday was pretty much a textbook example of a G-tube surgical procedure. Our daughter, Kathryn, left San Francisco early Thursday morning to drive to the hospital. She arrived shortly after we were taken to pre-op day surgery. I changed into the typical over-size hospital gown. The anesthesiologist met with us to discuss his plan—he would remain in the operating room (OR) on standby in the event he needed to administer anesthesia. Finally, the young, female, interventional radiologist carefully reviewed the procedure while allowing time for questions. I inquired about a MIC-KEY* (see below). Typically, a MIC-KEY is inserted several weeks post-op. The interventional radiologist said it was her intention, if possible, to insert a MIC-KEY during Thursday’s procedure. Success would be dependent on the thickness of my stomach wall and what size MIC-KEYs were available—they come in many sizes but not all are stocked in the French Hospital OR.
MIC-KEY*
Our MIC-KEY* Low-Profile Gastrostomy Feeding Tube is a step up from a standard gastrostomy feeding tube. When designing it, we listened to many enteral feeding consumers who requested a tube that would allow for an active and more mobile lifestyle. They told us it should be unobtrusive, easy to conceal under clothing and difficult to dislodge allowing freer movement.
Today, MIC-KEY* is the more mobile person’s ideal feeding tube choice. MIC-KEY* allows both children and adults to enjoy life to the fullest while ensuring their nutritional health and well-being.
An attendant wheeled my bed to the brightly lit operating room where I would spend the next hour. I was prepped for the procedure. They allowed me to have a pillow under my head to help me breathe easier while in the supine position. Throughout the entire operation, I was fully awake and alert but felt no pain as lidocaine was used to numb my abdomen. It was interesting and eye opening to listen to conversations among the surgical team throughout the procedure. During the final 15 minutes, the interventional radiologist said she was pleased she would be able to install the MIC-KEY as she had the exact size required!
Wheeled back to day surgery post-op to meet up with Jon and Kathryn, I was discharged just after 4:30 p.m. and back home within a half hour. There was considerable pain Thursday night and Friday, but that has become less intense throughout the day. We have been managing my pain with Tylenol and Advil, as needed.
Friday we benefited from the visit of a home health nurse. We are awaiting a delivery of supplies including liquid nutrition. This afternoon we were grateful for a second visit from a nurse on our home health team.
Thank you, each one, for your prayers and words of encouragement!
After considerable thought and discussion with Jon, I am scheduled to have a Gastrostomy (G) Tube (aka feeding tube) inserted via interventional radiology at French Hospital in San Luis Obispo this afternoon, November 21. Outpatient procedure. This past Monday morning, we became aware of a cautionary red flag involving the protocol utilized by our local interventional radiologists vs. protocol utilized by UCSF specifically for ALS patients with breathing and swallowing issues. The main issue of concern is general anesthesia v. less sedation and no utilization of oxygen. Late Monday afternoon, UCSF’s highly trained and knowledgeable respiratory care practitioner (RCP) phoned our local interventional radiologist and comprehensively reviewed UCSF’s recognized protocol. UCSF does not use general anesthesia for ALS patients when inserting feeding tubes nor do they administer oxygen.
We believe we’re “good to go” now. Your prayers for our peace of mind as well as care and skill for the interventional radiologist, anesthesiologist, nursing staff, etc. will be appreciated. Admitting time is 11:30 a.m., surgery set for 1:30 p.m., discharge anticipated at 4:30 p.m.
The purpose of the G Tube is to supplement my daily food intake. Eating is becoming more challenging by the day, exhausts me, and swallowing presents a possible choking hazard.
Please be especially mindful of Jon. This is more difficult for him than it is for me. He’s walked through many phone calls, deliberations, some frustrating miscommunication and/or lack of communication between medical professionals and/or their staff, long periods of silence when we’ve been left wondering, etc. He is exhausted while being concerned for his wife’s well being. He’s a trooper but I know it’s taking its toll.
My love affair with not just any hound—bloodhounds—started as a young, impressionable girl growing up in Sierra Madre. The small, charming community in southern California nestled beneath the San Gabriel Mountains is flanked by Pasadena on the west and Arcadia to the east. Every Fourth of July, the town hosted a festive parade on Sierra Madre Boulevard. Bloodhounds were always accompanied by the Sierra Madre Search & Rescue Team (SMSR). The high point for me!
While enrolled in third grade at Sierra Madre Elementary School, two classmates’ fathers served as volunteers with SMSR. One momentous day, both of those dads visited our classroom, magnificent bloodhound in tow. The men told us real stories involving their perilous work looking for missing hikers in the local mountains. Cell phones, GPS, and satellite communication weren’t even on the radar in the late 1950s. Bloodhounds, however, have been around for a verylong time.
A concerned mother would call the police (no 911 dispatch in those days!) when her son and his friends failed to return home as anticipated from a day hike in the mountains. The SMSR would be deployed to search for the missing boys. A boy’s dirty sock, baseball hat, or other unlaundered piece of clothing could serve as a scent article—something having direct contact with the skin. Every person is created with a unique scent. No two alike. The handler strapped on the bloodhound’s work harness, simultaneously sending a message to the hound saying, “We’re going to work!” At the place the boy was last seen, the handler presented the scent article to the bloodhound. Once the hound connected the scent on the article with the matching scent on the ground, the bloodhound immediately shifted from neutral into high gear and instinctively began hunting for the lost boy. Amazing! It’s just a fun game to the bloodhound. For humans, it can mean the difference between being lost or found. Perhaps life or death.
Have you ever had a pity party? Urbandictionary.com defines pity party as “A way of experiencing grief, in which you spend your time feeling sorry for yourself and whining endlessly about how crappy your life is.” Dictionary.com offers a slightly different twist: “A pity party is an instance of feeling self-indulgently sorry for yourself.”
You may have your own definition. Regardless, each one of us can experience hardship that elicits complex emotions. Life isn’t, as Mary Engelbreit suggested in 1992, “just a chair full of bowlies.” And pity parties accomplish nothing good.
You may have concerns about thieves breaking into your home and stealing precious things . . . family mementos, safeguarded coins, antiques, heirloom jewelry. Installing dusk-to-dawn, motion-detecting outdoor lighting; deadbolt locks; and security cams may thwart would-be burglars. But thieves come in many forms. Such uninvited pirates may show up at any time of the day or night to rob, bit by bit, our . . . health. The nerve! What have I hit on?! ALS ruins nerves! What does that look like for a victim of speech-onset ALS? A few personal glimpses:
Diminished ability to speak
Difficulty chewing
Swallowing—even liquids—can be hazardous
Excessive saliva results in drooling
Weakening diaphragm causes undue fatigue
Ordinary tasks take an unreasonable amount of time
Jon often reminds me to be thankful for what I still have left. Pivotal. Otherwise, it’s tempting to wallow in what I’ve lost.
Please thank Godtoday for your many unearned blessings. And when you take a bite of that In-N-Out burger or turkey thigh or pumpkin pie, chew and swallow it, be grateful. Something as seemingly insignificant as that shouldn’t be taken for granted.
So glad you’re here! Heartfelt appreciation to our daughter and son-in-law, Laura and Jarrod, for sharing their expertise in designing this website from their home in Chattanooga, Tennessee.
Thank you for your concern expressed through emails, texts and cards and for your prayers. An appreciable decline in stamina makes it difficult for me to keep pace with individual emails and text messages. My hope is you’ll return here for current news and personal reflections. You’re welcome to email or text me but no promise you’ll receive an individual response.
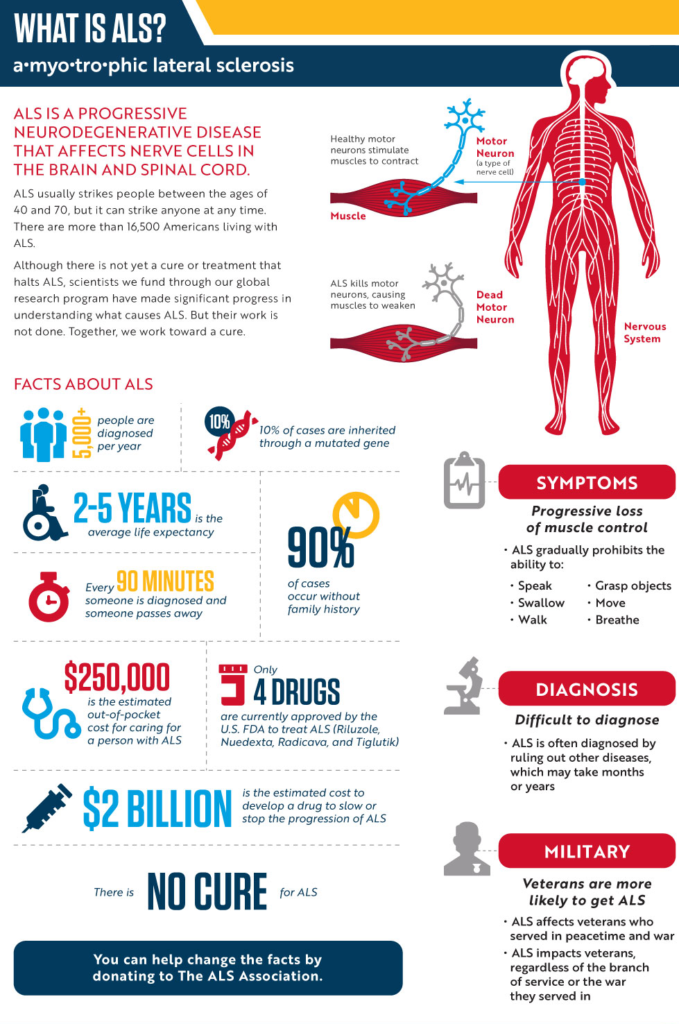
Amyotrophic lateral sclerosis (ALS), also called Lou Gehrig’s disease, is a progressive neuromuscular disease that weakens and eventually destroys motor neurons— components of the nervous system that connect the brain with the skeletal muscles.
Upper motor neurons are located in the cerebral
cortex of the brain and conduct impulses from the motor cortex to nerves in the
brain or the spinal cord. Lower motor neurons are peripheral neurons that
originate in the spinal cord and conduct impulses to the skeletal muscles.
Skeletal muscles are involved with voluntary movements, such as walking and
talking. The lower motor neurons transmit the command to move from the brain to
the skeletal muscles, which respond by contracting.
A person with ALS usually presents with problems in
dexterity or gait resulting from muscle weakness, or with difficulty speaking
or swallowing. Sphincter control, sensory function, intellectual ability, and
skin integrity are preserved. Patients become paralyzed and often require
ventilation and surgery to provide a new opening in the stomach (gastrostomy).
Loss of respiratory function is ultimately the cause of death for people who
have ALS.
Incidence and Prevalence of ALS
Approximately 30,000 patients in the United States currently have ALS. The disease has no racial, socioeconomic, or ethnic boundaries. The life expectancy of ALS patients usually ranges from about 3 to 5 years after diagnosis.
ALS is 20 percent more common in men than in women. However, with increasing age, the incidence of ALS is more equal between men and women.
About 90 percent of ALS cases occur without family history. The remaining 10 percent of ALS cases are inherited through a mutated gene. On average, it takes about one year before a final ALS diagnosis is made.
ALS signs and symptoms
Once a motor neuron
degenerates completely, the muscle that it controls no longer receives impulses
from the brain. Approximately 60 percent of ALS patients experience muscle
weakness and stiffness as the initial symptom.

 You would highly regard our five-star Central Coast Home Health RNs. Such caring, confident, calm, and competent professionals who put the needs of the patient first.
You would highly regard our five-star Central Coast Home Health RNs. Such caring, confident, calm, and competent professionals who put the needs of the patient first. 



 My love affair with not just any hound—bloodhounds—started as a young, impressionable girl growing up in Sierra Madre. The small, charming community in southern California nestled beneath the San Gabriel Mountains is flanked by Pasadena on the west and Arcadia to the east. Every Fourth of July, the town hosted a festive parade on Sierra Madre Boulevard. Bloodhounds were always accompanied by the Sierra Madre Search & Rescue Team (SMSR). The high point for me!
My love affair with not just any hound—bloodhounds—started as a young, impressionable girl growing up in Sierra Madre. The small, charming community in southern California nestled beneath the San Gabriel Mountains is flanked by Pasadena on the west and Arcadia to the east. Every Fourth of July, the town hosted a festive parade on Sierra Madre Boulevard. Bloodhounds were always accompanied by the Sierra Madre Search & Rescue Team (SMSR). The high point for me!